This is a catch all area
 There have been a lot of interest on the GDPUK website recently following the publication of the death rate of dentists waiting for fitness to practice hearings. This is the latest response as published in todays Times. As an individual dentist we are vulnerable, we should have some form of united response in a similar manner to Dr's who are better organised for similar problems with the GMC. The GDC should protect us as well as the public. Read on. What are you going to do? Follow the articles on the GDPUK site.
0 Comments
Are you happy with the teeth4life App? Would you please complete this one minute survey to help me improve the App's content?
FEEDBACK It's just over a year ago since I retired from clinical dentistry. I have wasted the last year trying to engage the NHS AHSNs, and ORCHA to help improve and help fund the App, more importantly, the awareness of a free, trustworthy oral health prevention resource for the public and the profession. While the government has a "prevention is better than cure" policy, there is no evidence of funding for dentistry in any NHS innovation accelerator programme. With the SOP restrictions, I felt I had more to offer, trying to improve the dental health of the many people we can't see through marketing the App. Like most Apps you use, it will improve iteratively and with feedback. It will need an income to maintain the current freemium version for most DCPs and the public. From January 1st there will be a charge for dentists as we benefit most from advertising our prefered procedures on our profile. Used correctly, as outlined in the registration site care4teeth.co.uk it saves you time, promotes your more profitable services, and provides some protection against periodontal litigation. This is the five minute Pitch video I have made for the profession regarding marketing. It's your choice to use the time saved to earn more money or do something else you enjoy. PITCH FOR DENTISTS In the future, we can have a white labelled template with the ability of the DCP to personalise the content a lot more it would benefit from some input from DCPs starting their career, not finishing it. I need to interview about 20 DCPs to get further insight into what you want in a future premium version to engage the profession more. You would get any future premium version free for life. I made the App based on what I think the public need concerning prevention advice, to market it better, I need to know what you and the public want. If the App is successful, I prefer a For-Benefit Enterprise model for the dental profession as a whole and build a team to collaborate and organise small groups of interested parties, like the peer review group I organised for ten years before covid. Ultimately, we could develop a legacy business model or scheme to support dentists and be prepared to provide a service for the majority of people when NHS dentistry fails. We can't do it as individuals, but as a group, we have a chance if we collaborate and share our ideas and experience. Would you please get in touch if you want to help? And if this isn't for you, please forward it to someone you know in the profession who may want to help. I retired from clinical dentistry last year and spend a lot of my time thinking of how we can improve our health delivery. While there have been many advances in dentistry, when it comes to checking if our teeth are clean, disclosing still works best. Unfortunately, it's a bit too cheap to get much recognition. However, when it comes to research, there have been 3270 papers written on the subject, and a Cochrane review recent paper concluded that only one was of value.
https://www.nationalelfservice.net/dentistry/oral-health-other-health-conditions/plaque-disclosing-oral-health/ So with my simple maths, if extrapolated, it means of the two million research papers published each year, less than 700 are of value. To progress in academia, you need to get published, and there may be a conflict of interest here? I like conspiracy theories, and I've wondered why we can only get one make of toothpaste on prescription in the UK? There are far better products and have been available for many years in different countries. I came across Clinpro 5000 in Las Vegas six years ago at a digital dentistry conference. Now we have an innovative toothpaste Biomin available in the UK, with FDA approval but only on prescription in the States. We are still investigating rather than implementing silver diamine fluoride in the UK when we are fully aware of its benefits It is used in the USA, Canada, and has been used in Japan for over 70 years. Do we have different teeth? There is some movement on fluoridation, but it has been regularly reviewed ever four years for the last fifty years. The evidence is there, but no political will. Let's continue to traumatise the children with increasing GA sessions at a cost to the NHS, us the taxpayer, of billions of pounds, which is nothing compared to the mental trauma of the child and their parents to a potentially life-threatening procedure. Unlike covid, we will never be vaccinated for gingivitis or caries. However, when it comes to prevention of the worlds most common diseases, why do we have these barriers? There is a lot of discussion about the link between oral health and general health. This was more an observation. https://www.efp.org/news-events/news/jcp-study-shows-that-periodontitis-is-linked-to-covid-19-complications-30539/ The pharmaceutical industry has improved since I listened to my audiobook on BadPharma. Unfortunately, even google is struggling to find the relevant paper regarding a future study on the relationship between general health and oral health I read recently. And that to avoid the three-quarters of poor outcomes which were never published, the research criteria is such that the method is issued prior to it being implemented. A recent paper I read, but even google can't help me with this morning, was on the oral and general health link. The parts that struck me were the study required irrigation of the pockets with GSK chlorhexidine, while all the other cleaning products were from Colgate. I had a "Cavimed" years ago which applied the chlorhexidine directly in the pocket. I stopped using it when new research demonstrated the results showed only a transient effect. One can only conclude that the research will show a result that using these products improve general health. We can imagine the marketing campaign that is already written. Yeara ago, I discussed with a Professor of periodontology my idea of oxygenating the periodontal pocket with ozone using suck down splints. Even I knew it would never be possible. It must have been after the Legionnaires scare, and I asked about the safe concentration of hypochlorous acid in a pocket through a standard ultrasonic, and sodium hypochlorite. His answer was no one knew, as hypochlorite was too cheap for the research to be funded. Well, we know now. This is one of many recent obscure papers. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6906904/ Now again with my simple maths, how much hypochlorite is required to irrigate the root canal? The most viewed TedTalk is by Sir Ken Robinson. It explains how through our training, we may stop being curious and now have a different view. https://www.ted.com/talks/sir_ken_robinson_do_schools_kill_creativity?utm_source=tedcomshare&utm_medium=social&utm_campaign=tedspread Many GDPs my age are relieved to retire due to the external threats that create unnecessary stress, which, as we are aware results in poor performance. My vision is to create an eHealth product Promoting Public Prevention in oral health for the public and reducing GDPs' stress. The free teeth4App could help reach the 48% of adults who don't visit a dentist regularly and give preventive advice through videos. The videos in the teeth4life App has about 60 videos based on my forty years of experience and my CPD. It would be far better if it were a collaborative effort endorsed by a professional body rather than a business whose main priority is profit for the shareholders rather than the health of public. The App has a scoring system devised by the evidence from some of the dental health research papers already published. It is not perfect, it could be improved, it will never be 100% accurate. It does give a reasonable indication of oral health in a traffic light system, and more accurately, the risk of oral cancer and how to monitor yourself for this sixth most common cancer. Like all cancers, early diagnosis is the key. I have had a lot of contact with AHSNs and Orcha. My App will never get a rating to be "approved" by Orcha unless I remove the traffic light system which indicates the risks above. If I remove the scoring, it will pass. It will be good enough from the criteria set indirectly by NHSx, but serve little value for the general public. I have been advised to carry out some research to justify my figures, they can reevaluate it. And they recommend I will have to make it self funding, therefore charge for it. If we make a viable version and engages the public and is financed by some of the profession, then the profession should take the credit. I think we can make prevention work, but we have to engage with those outside academia and those with a skillset outside dentistry and ask simple questions for simple answers to help improve all our wellbeing. The biggest dental corporate had hindered rather than helped oral health over the last twenty years. There is a better alternative, we just haven't thought of it yet. Please help. Published by Status is online Tony Smith Dental Entrepreneur promoting prevention for both the public and the profession through FREE eHealth product Published • 1w 3 articles hashtag#preventionisbetterthancure hashtag#healthawareness hashtag#dentalhygienist hashtag#dentalbusiness hashtag#buisnessideas hashtag#innovation hashtag#appdevelopment hashtag#dentistry hashtag#videomarketing hashtag#marketingcontent Like Comment I was asked by a dental Magazine to write an article about the App, in the format of answering their questions. This is it:-  What is Teeth4life? Teeth4life is an eHealth product. It's a free resource available now to download on the App Store and Google Play. It protects us with the data stored on our dental software, and promotes our services with a customised profile. It has a scoring system to monitor oral hygiene and has a notification centre which ideally, following your advice, supports them in creating and maintaining good oral health. It encourages the user to take ownership of their health through gamification. The default advice should recommend a monthly reminder for oral cancer and get in the general habit of self-monitoring their health. Never have we been more aware of the poor outcomes if our general health is poor. As general health is directly linked to oral health, why not also use this opportunity to educate them on preventing the world's most common disease? You can customise the App for free via the supporting website care4teeth.co.uk. Please read the section on marketing and the blogs on support. The public can select your details from the MY DENTIST section and personalise it for themselves and their family in the MY TEETH section. Please give us your background, how did you come to creating this app? I was lucky as I moved to Anglesey when I was six and went to a comprehensive school. None of my 26 cousins did, and I was the first to take A levels, partly because I was too young to leave. I'm the only one to go to university where I could have studied science, which was my strength, but instead studied dentistry, as I remember my Dad stating, “But dentistry is a profession” and back then, I wanted a job. I liked the idea of being my own boss, helping people, and never having to be on call or open a book after qualifying, unlike doctors. It was a long time ago! As a profession, we have ethical and moral obligations and need to warrant the public's trust at large. I am concerned that, like many professions are we are being hijacked by big business. The purpose of a business is to create and keep a customer. Until I sold my practice to a corporate, the patient was the customer. In effect, I became the customer and "my patients" become a commodity for the accountants that run these businesses. Just as the government can complain about Vodaphone and Amazon's tax dodges, we struggle with large dental corporates and AI-driven orthodontic groups who take the income but no responsibility for the outcome. Sadly, after nearly forty years as a GDP I don't trust the government to promote dental prevention. When I have approached the NHS with the App, they have asked me how it will generate money for the NHS. The bureaucracy is so big it has lost its founding principles of "universal, equitable, comprehensive, high quality, free at the point of delivery, centrally funded". As a profession, we are obliged to do it ourselves. I sold my practice around the time of my Dad's declining health which resulted in his care for over a year in a dementia ward, where oral hygiene was difficult. Many of my patients were carers, and I asked them about their experience and subsequently made a website care4teeth.org to support them with a variety of resources, including video links I thought useful on YouTube. Technology changes, and while the now redundant iPod carried 10,000 songs in your pocket, any smartphone can have you in your patient's pocket, well, at least your advice, and while they are in the bathroom cleaning their teeth and gums. I approached a few dental App companies, but they used basic retail templates. Many large companies have Apps, but in the main as a vehicle to sell only their products. There wasn’t an impartial one that covered most aspects of preventive dentistry and so eventually, I thought I'd make my own. It has taken a while as the first App company I was going to have joint venture with wanted to charge the public, and would be a hurdle for the public I was trying to engage. I eventually designed the App that as a dentist I would find useful, and eventually used a small company to produce it, while I gradually taught myself to make videos, via YouTube.  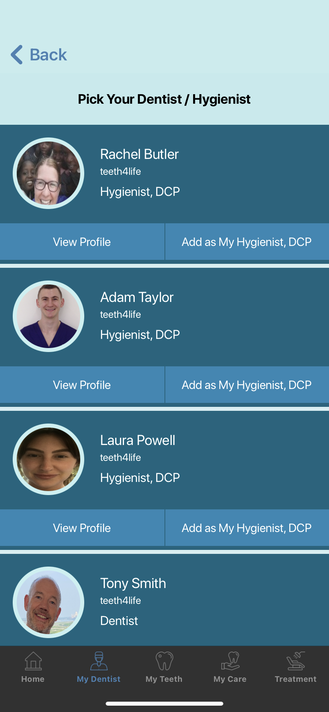 Who is the app for (eg what dental practice would benefit from this? The App is for two main groups. It's a template for individual dentists and hygienists who can register and learn how to promote and protect themselves as outlined here care4teeth.co.uk . It is also for the public, our patients, and the 50% of adults who rarely see us. They may contact a dentist registered on the App after downloading and using the App themselves. It can easily be shared using social media links on the user's phone. The embedded short video animations are for the public as few of us to read pamphlets anymore. I am anticipating some criticism especially in the TREATMENT Section. I have only ever regarded myself as a good GDP, not an animator, and if there is constructive, consistent feedback I will update the videos. The App will then improve in each iteration. If you don't like the audio or content, I advise on how to change the video content yourself on the supporting teeth4life YouTube Channel, and email your patients directly. Lots of my original videos are there, but the recent feedback was animations with audio work better. Please subscribe to the YouTube channel, as then more members of the public will find the App. An email template in your practice software similar to this should help you sleep better of a night. Dear Bill, Following your appointment today. These are your scores. BPE 11112 BEWE 010111 Download our free teeth4life dental App available on the App Store and Google Play. Press SQUEEZE ME on the tube of toothpaste on the front page to see how the App works for you. Personalise the App in the My Teeth section, add your scores and risk factors, then view your scorecard. Set appropriate reminders to help improve habits. Select me from the MY Dentist section, and check out the molar apicectomy procedure I recommended for your lower left second molar tooth in my profile section. This animation explains how oral health is directly linked to general health. Keeping your scores in the green may well help maintain your immunity, as well as a healthy smile. https://youtu.be/9Tbp6zi7wnc Please look at this animation video on Oral Cancer as you need to monitor yourself for this largely preventable, and deadly disease. There is a shorter self monitoring clinical video in the App. https://youtu.be/9IzyuFDpHUY Set a monthly reminder in the My Teeth, scorecard section. Please share the App link with family and friends from the social media icons on the front page. Help save a life SHARE teeth4life. Stay Safe, Your Best Dentist in the world  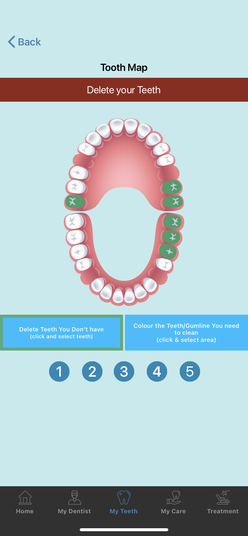 How many practices are using it at the moment? There are around 350 dentists and hygienists registered on the App in the UK, and it has been downloaded a few thousand times worldwide. The current iteration on IOS version 1.4 has a global location finder, but there have been significant changes in the IOS software, and another update is required, so it is best as a user to delete the old software and reinstall as often is required for all Apps. A year ago, I was in India during their lockdown. I realised quite a few of the public there didn't see a dentist, but they do have smartphones. And most have teeth, so it wouldn’t cost anymore for dentists to have the App there, or anywhere else with a signal. What is the cost to dental practices? There is no charge for the individual dentist, hygienist, or dental therapist, and it will always be available for free in its current form. I’m well aware that not all dentists can afford the Latest Porche as our patients think, it has to be free for it to be shared. In the long term, it would need to generate some income to maintain and improve what has only recently moved on from a minimal viable product to a functioning eHealth App. In the future, there could be a charge to customise the front page, and that would be more appropriate to practices, but it could apply to individuals. While I could populate it with adverts like Spotify, I think the public would find it irritating. It could be that there was a shopping basket of preferred products advised by the dentist, and this could generate some income. Or further chargeable customisation options, or chargeable global notifications. There was no charge as an MVP, as I was still working and charging was too time consuming. Most dentists were happy to pay £5 a month when I demonstrated it at the dental showcase, but one dentist offered £600-700 a month to be first on the location finder. So I probably ought to investigate this. I was also funding it with my NHS pension, but I have now retired, so it will soon need to be self-funding in the future. It’s interesting that Wikipedia, and TedTalks both of which I’ve used for references, are now asking for donations.  Anything else you’d like to add?
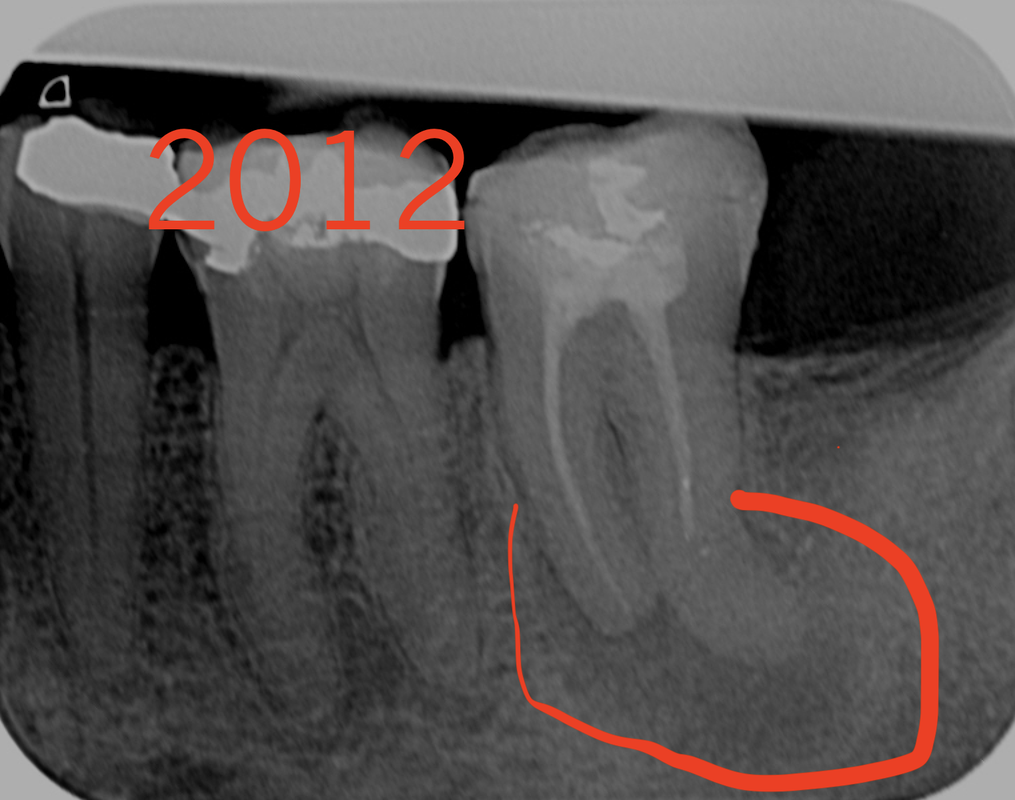
Bored with NetFlix try DenFlix? I have recently registered the domain denflix.co.uk. It could help all dentists as a single go-to resource if we all collaborated and left our egos outside the Zoom door. I can't be the only retired dentist who enjoyed prevention, MID, and trying to help the public keep their teeth4life? This is somewhere we could all help one another. I've started to set it up primarily for FDs as a mobile webpage. There is a Gold section for procedures without the limitations on time, materials, and equipment to help everyone improve their specific skill base for free. Last year the CDO mentioned CVEK and silver diamine fluoride in the SOP. But now the discussion is 45% activity, which is still mainly the cure, not prevention. Look up, denflix.co.uk on your phone. On the menu, press Procedures, Bronze, Child and view in landscape. Watch Dr Jeanette MacLean's excellent video on silver diamine fluoride. It makes you think. There is also the one on CVEK, which took a while to find. Perhaps we all need to think and act a bit different? Download teeth4life and press SQUEEZE ME on the front page. It explains the pre-covid tag. Save a life, SHARE teeth4life. Even better customise the App for yourself, via care4teeth.co.uk. This weekend I've been thinking of the problems FDs and their trainer have due to covid. The Fds will have less experience coming out of dental school than ever, which adds to the pressure on both the Fd, and their trainer. then at the end of their FD year, they will still be relatively inexperienced compared to the past. This was an idea, that could work with collaboration. DO you want to help? CLICK HERE for the page link.  I've written the outline on this site. It's for FDs, but also there could be another section as a resource for dentists wishing to upskill. The idea that we don't get lost viewing poor videos, and spend our time more effectively viewing a good resource selected by our peers, on our phone in work. Use the saved time, restoring our work/life balance at home. 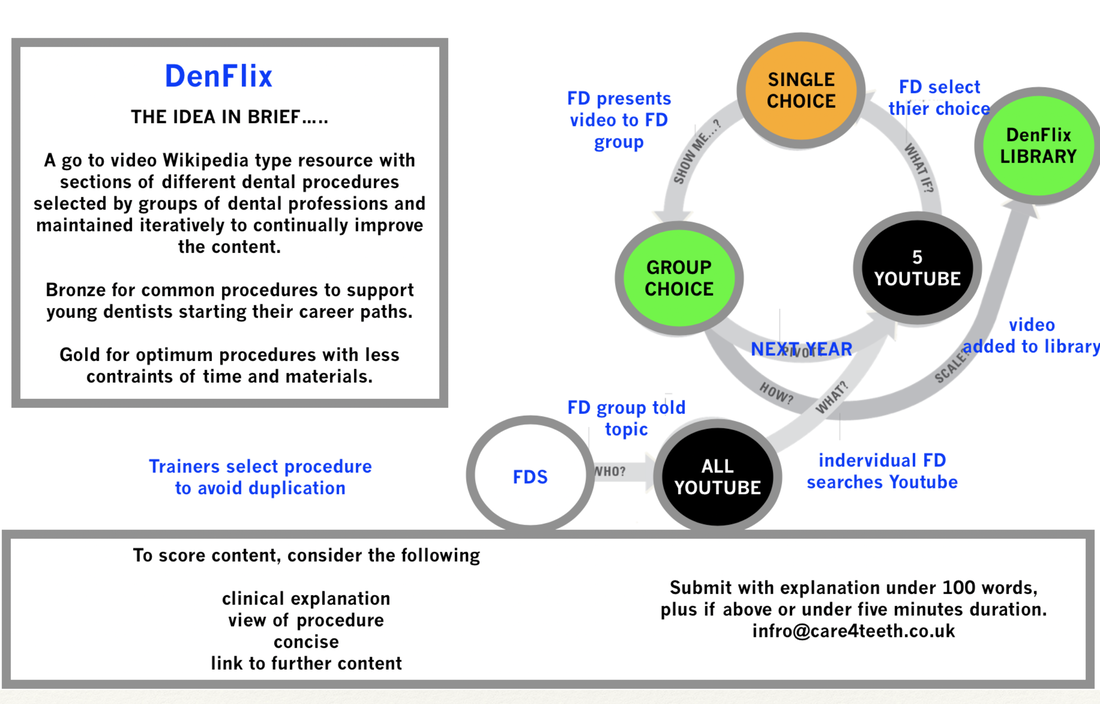 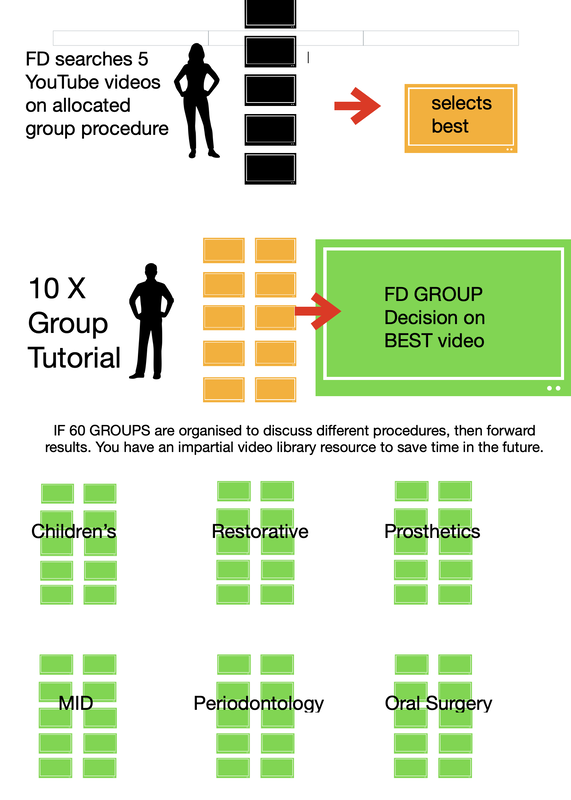 Covid has impacted all aspects of dentistry, and the impact on training is probably most significant. What can we do to support those embarking on their career? The burden on trainers is greater than ever, and we need to support them as much as the young dentists. The financial rewards are not sufficient to warrant training, and it's often a vocation. But let's hope everyone is getting the support they deserve or highlighting it to those who have influence. 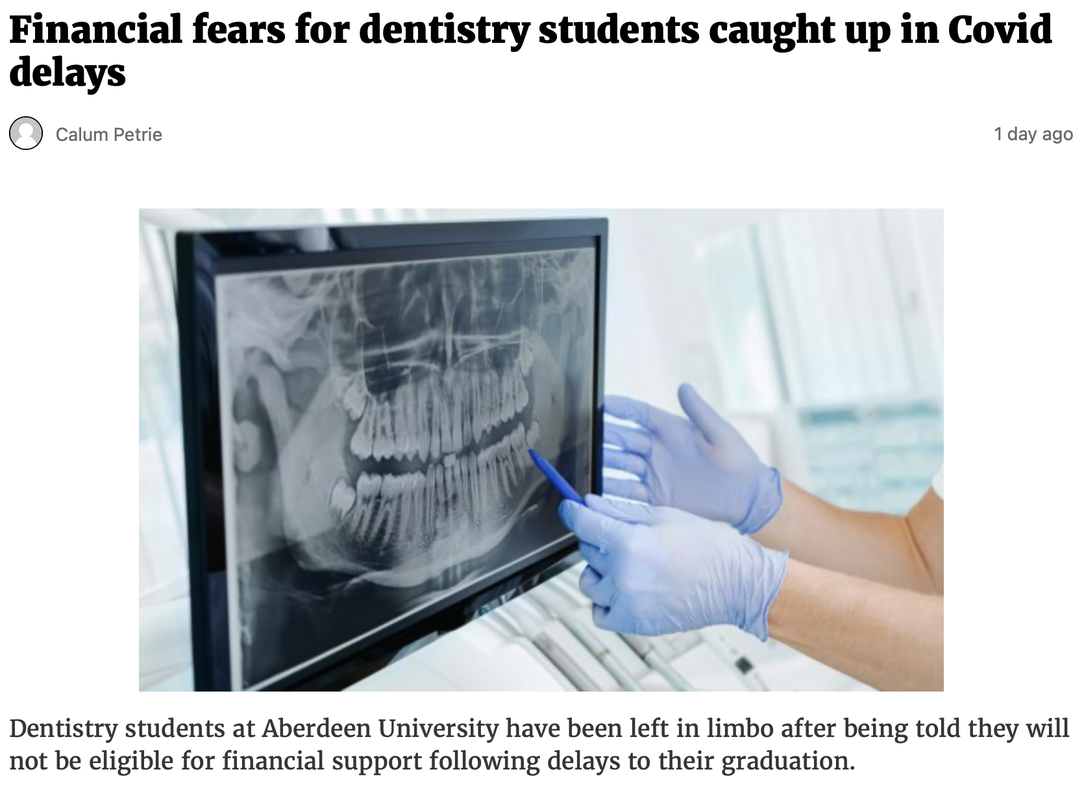 click on images for further articles.  Interesting isn't it - having an 'extra' year can esure additional opportunities and competency reinforcement, rather than compromise or gaps affecting every year perhaps Many have been suggesting 2 years FT/VT to improve clinical and professional skills on the front lines for years pre-Covid, as graduates have gradually had less and less patient treatment opportunities chronically - there are some exceptions of course but the chronic trend has been there for years, thus the fudges of counting any root-filing as say filing a canal in one patient and obturating only in another, as being valid beginning to end competency achievement - indeed it is not unusual to have FDs say in February this is my second ever amalgam restoration, after graduating from Dental school. Some have done double figures, some done non, it is that variable So who knows, with undergrads getting even less clinical exposures, less support, less confidence on graduating (from less staff and less resources to teach by the way, they are rationed too) and only 1 year if FT/VT to help most survive in a Practice setting, perhaps an additional funded year is an investment in them and the Profession Or how about this for a radical thought - extend the Undergraduate course to 6 years and qualify it as a proper University Doctorate, DDS or DMD, like most of the rest of the world ie: a proper Doctor title, not honorary, just like Hungary, Sweden, Portugal, USA etc, etc I suppose one could counter-argue they'll lose 1 year of 'extra' earnings in a 40+year career; but also what are the odds of them getting an early complaint or GDC sanction or worse, if they have even less proficiency and experience clinically etc - will they end up more vulnerable or stressed or even cutting their Career short in our very adversarial systems currently ?!? Whatever the Dental Schools produce/graduate, Foundation Training is legally obliged to try and make the best of it, but given Dental Schools have the person for 5 years, the scope for FT/VT to compensate for any under-developments is only 1 year for most (some 2 years schemes exist and they are excellent wrt professional development outcomes) and thus 1 year gives very limited opportunities. Having said that our Trainers and HEE and the Practices that support them do an amazing job, but ultimately they are not miracle workers and neither are our Undergraduate Teachers and thus...... is an additional year for all, the optimum smart outcome here I'm guessing this qualitative aspect was a major factor in Scotland's decision to add a year but as always, those who control the purse strings decide - if it was down mainly to the quality of the Professional produced for the next 40 years, for many the decision would be a no-brainer I suspect. A piece of research from Qatar was on Twitter at the beginning of the month. Click on the picture for the link.   This follows up the research carried out in Birmingham by Professor Iain Chapple and his team published in January. I have seen him lecture twice on the subject, and still, I couldn't quite understand the exact mechanism of the link but grasped the method. He used some excellent video animations to explain the process. I made an animation over a year ago to present it to my patients so they may understand. I'm not sure if my explanation is accurate following Qatar's research, but the outcome is the same. I think it is called a "Plato's truth". While my information is not 100% accurate, the message is for the benefit of the recipient. It also may be funny, and laughter is the best medicine. New Year has brought in some further clever advances in software. I used this software a few months ago while I was still working in Practice. My GDC registration was not updated, and so I assume I am able to voice my opinion without losing my livelihood. Our dexterity will always be required, but we will find it easier to communicate with our patients in a targeted fashion. This was made in September, and it's still in Spanish. I added one image, the rest were chosen by AI, as was the language. I struggle with English. Its my best language, I have no idea if this is Spanish, let me know if it isn't. This is the software it was made on with the text used translated into Spanish. The software choses an appropriate image, and the language using the text which may have been via speech recognition. If you can't read the text, then this was my first attempt. I have heard my voice is too monotonous and dull, so using AI I had a sex change. Click for the animation, in English. There have been some further developments with all software, but teeth and gums are the same. Please download the teeth4life App. Customise it for yourself to help promote and protect yourself. Let's make 2021 a year when we were able to promote prevention in health, and take back control of our own work life balance. This is a link explaining how the teeth4life App can promote and protect you. In the USA a 1951 policy on water fluoridation enabled 74% of the USA to access fluoridated water by the time when I qualified in the early 1980's. The prediction was that by the year 2000 decay in children would be irradicated. This never happened. Instead, as in the UK, where currently water fluoridation is only 11%, and despite the increased explosion of marketing of toothbrushes, toothpaste, and mouthwashes, it didn't work. How come? Why won't it work in the future? What can we do? As you can see around 1990, the decay rate plateaued. It explains why with our 11% of fluoridated teeth, the decay rate in the uk is worse, and from the last review in 2019 increasing. The graph is taken from the dentist below who qualified ten years before myself, and voicing an opinion similar to my own, and a lot of GDPs. Click on the picture for her enlightening presentation.  We need to integrate our health delivery to the public in a different way. It is so disappointing to retire when our knowledge is greater than ever, but by any standards our results are so poor. We have failed because we work in isolation, and as everyone knows you need to get in a helicopter and take time out from dealing with indervidaul decay, and see we are a small aspect of health. The governments green paper states the following regarding the savings for prevention for the under fives. For the general population the average is now a £14 saving.  This is all the evidence we need, I don't think anything has changed. Why procrastinate? 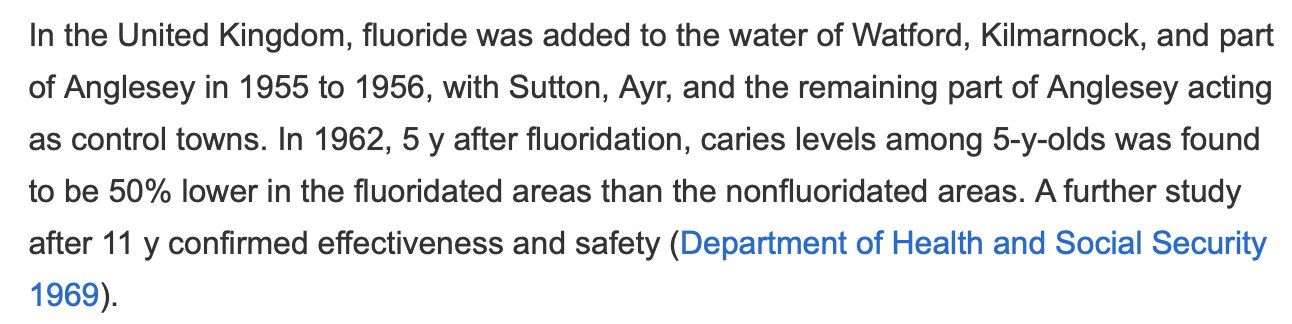 When I moved to Anglesey in 1996, water was fluoridated, but a bit late for me to have the maximum benefit. In 1992 Welsh Water unilaterally withdrew the water's fluoridation, and the dmf rate more than doubles in a five year period. The public, and the profession were not informed. The evidence is there. Just Google it. https://journals.sagepub.com/doi/full/10.1177/0022034519843495  A BHAG I remember from years ago in the early 1990's, before I had a computer at work. It's a Big Hairy Audacious Goal devised by Jim Collins. I didn't know it was attributed to him then, but I googled it. More recently I came across OKR on a Ted Talk. Objectives, and Key Results. The objective or goal in my lifetime has never changed, its prevention in oral health. I always found it depressing having to restore childrens teeth, listening to parents telling me their children ate too many sweets. Occasionaly, when brave, I asked where they got the money. My results were satisfactory, but nationally my gut feeling is we are worse. A lot worse, as outlined in the excellent presentation by Marielle Pariseau, with some insight in how to overcome it. A famous quote attributed to Eintein was " the definition of insanity is doing the same thing over and over expecting different results". Governments regularly publish results, such as childhood GA extractions and obesity. Similar for adults, but at this age, our prevention focus should be on their "gums". Let's try something different. The government paper on "Advancing our health: prevention in the 2020s" from July 2019. prevention mentions targetting the under 5's only with OHI, and water fluoridation (page 51 gov paper prevention). In the PHE report on water fluoridation from 2018 on page 8 Water Fluoridation: Health monitoring report for England 2018 Conclusion The findings of this report agree with the view that water fluoridation is an effective and safe public health measure to reduce the frequency and severity of dental decay, and narrow differences in dental health between more and less deprived children and young people. and then on page 14 of the 135 page document. "PHE continues to keep the wider evidence under review and will consult with local authorities prior to publication of a further report within the next 4 years. " Why support water fluoridation? Fluoride in water can reduce the likelihood of experiencing dental decay and minimise its severity and is the only intervention to improve dental health that does not require behaviour change by individuals. How this programme can be implemented at scale Since April 2013 the power to make new proposals to establish, vary or terminate water fluoridation schemes sits with local authorities. There are a number of local authorities currently considering water fluoridation. Although decision making lies with the local authority, local partners such as the NHS have already been integral in supporting plans for proposals. The intervention has been included in PHE's return on investment tool for oral health. The PHE return on investment tool can be found on the gov.uk website. Based on the average dmft (decayed, missing or filled teeth) for 5-year-old children in England (national oral health survey of 5 year old children in 2013), the return on investment tool suggests for every £1 invested there is a £12.71 return on investment after 5 years and £21.98 after 10 years. This includes savings to primary and secondary NHS services. source https://www.england.nhs.uk/ltphimenu/better-care-for-health-conditions-for-dental-healthcare/dental-care-and-water-fluoridation/ 3/12/2020 Root fillings, can wE accept good outcomes from imperfect treatment, or not even try?Read Now When I qualified, we used endomethasone for root fillings, as SPAD was a bit toxic. I remember an article on a review of the 100% success rate of endomethasone being spun through the apex in anterior teeth of 24 RAF personnel. This is the closest paper on a comparison with laterally condensed GP I could find. It's from my dental tutor who is the current president of the European Society of Endodontology. If I was good at statistics, I'd say there was no difference, but perhaps we ought to contact the ex RAF personnel and advise they have their teeth removed in case of a potential problem. Fortunately, I never witnessed an air embolism and in all my time, I never seem to have extruded any hypochlorite. The best advice I received was in the pub about twenty years ago from a physics PHD student who was writing his thesis on the movement of fluids in confined spaces. Fluid always follows the path of least resistance, so unless you have jammed in your needle or not in the pulp chamber, it should be safe. Once the hypochlorite is visible around the needle, why put in any more. There will be displacement when you place your rotary file. The excess will flow into the floor of the access cavity. Applying more pressure when applying the hypochlorite at best fills up the access cavity, and at worse could extrude. Why bother? The files should carry the hypochlorite around the root canal surface. There is no need to fill it. I used to wash out the hypochlorite with hypochlorous, and if you could dry the canal, I'd fill it.  As you wash with a 3 in one and high volume suction, and air dry over the tooth, then cotton wool balls and paper points. I didn't get an air embolus which was a real concern for about twenty-five years of my practising life, and far more likely on those complicated extractions when you had to separate roots. And it would seem if ever there was any loss of the hypochlorite into the oral cavity, it would be rapidly less than 0.2%. So apart from the taste. No harm done. I know of crowns being at best swallowed, and worse inhaled—the same with bristle brushes, teeth, and rubber dam clamps. Last year I saw a patient as an emergency as he woke up one morning with something in his mouth. He handed me his implant. It definitely wasn't one of mine. I don't do implants. We used a rubber dam for hand files. Am I the only one who never uses hand files, everything is rotary and firmly attached to my reduction handpiece? I take a working length with Gp Points, and the preformed GP isn't quite the same as the GP we used in the past. The results I had over the last ten years were as good, and probably better than with silver points, or Gp placed with endomethasone in the 80's.
I used thermafill about twenty-five years ago and like a few other dentists I know, found while they looked great on the radiograph, the patients didn't like them. Or put another way they had poorer outcomes, than with a single preformed GP point. If you want to fill some lateral canals, then smartseal seems to fit the bill. I had success with this. But we will never clean all the pulp tissue, we just need to clean enough. How much is enough? In my experience it seems to vary from person to person. A bit like the reaction some of the public have to covid. I clearly am not a specialist endodontist, I was a GDP and I was at an age where if a root filling failed, and a patient complained, and an expert witness said I'd missed the 2mb canal, or a lawyer said the notes didn't have the expiry date of the Gp on. I would have done what the defence organisation would advise, and give the patient their financial compensation. And I would have retired. The three radiographs above could make up a few more blogs.
This is in the Ethics section. So is it ethically right that we are passively deskilling to protect ourselves. The reason to work is to stretch ourselves, not to refer to some non-existent NHS specialist. We need to change our health delivery system to help the public, and start to enjoy the career you trained for. |
Guest authorHave something of interest to share. this may be the place Archives
June 2023
Categories |

 RSS Feed
RSS Feed